Understand Australia
About Australia Covid booster shots
Severely immunocompromised Australians will be able to get Covid-19 vaccine boosters from Monday, after Australia’s vaccine regulatory body approved the jab for the vulnerable section of the community.
In advice released on Friday, the Australian Technical Advisory Group on Immunisation (Atagi) recommended the third vaccine dose for all people aged above 12 who either have conditions that severely weaken their immune defences, as well as patients receiving cancer treatment and other therapies.


The government expects about 500,000 Australians to be eligible for the initial rollout of booster shots.
However, not all of the older Australians who were first to receive vaccines in early 2021 will be eligible for the early booster shots, and it’s less clear how and when boosters will be administered for the rest of the population.
Here is everything we know about Covid-19 vaccine booster shots.
Definition of severely immunocompromised
Having a weakened immune system. People who are immunocompromised have a reduced ability to fight infections and other diseases. This may be caused by certain diseases or conditions, such as AIDS, cancer, diabetes, malnutrition, and certain genetic disorders. It may also be caused by certain medicines or treatments, such as anticancer drugs, radiation therapy, and stem cell or organ transplant. Also called immunosuppressed.



So who is eligible?
When announcing the booster program on Friday, chief medical officer Paul Kelly said the severely immunocompromised group would include people who were already seen in phase one of the vaccine rollout to be priority groups.


chief medical officer Paul Kelly
“So, people with active blood malignancy, blood cancer, people with other types of malignancy as well, people that have had organ transplants, people that have had stem cell transplants, people on immunosuppressive therapy,” Kelly said.
“There are people … who have had transplants that have medications to dampen their immune system. But there are others on certain types of arthritis medication and steroids, for example. Those that are born with immunodeficiency, there is a group of those as well as people that are living with HIV who are not controlled under therapy.
If I’m eligible, when and where do I get it? Is there a recommended interval between the second and third dose?
You can book your third vaccine from Monday if you’re eligible, and receive it from any of the settings already participating in the rollout. The recommended interval for the third dose is two to six months after their second dose of vaccine.


Do I have to get the same type of vaccine as my first two doses?
It depends. The Atagi advice is that third doses are of an mRNA vaccine – which are currently the Pfizer or Moderna options.
If your first two doses were of an mRNA vaccine, Atagi recommends sticking with the same vaccine type for your third. For example, if your first two doses were Pfizer, you should get Pfizer for your third dose.
Kelly also said that, in the above example, if Pfizer is not available, Moderna can be substituted, and vice versa.
If your first two doses were AstraZeneca – which is not an mRNA vaccine – the advice is for your third dose to be an mRNA vaccine.
However, Kelly said there may be certain circumstances where you need an AstraZeneca vaccine as your third dose, giving the example of someone who had side effects after receiving a second mRNA vaccine.


Who will be next in line? And when?
Health minister Greg Hunt said the government is expecting advice from Atagi about the general population’s stage of the booster program “before the end of October”. The government will consider advice for health workers, as well as people with less severely compromised immune systems.


Health Minister Greg Hunt
There are likely to be further stages of eligibility which correspond to eligibility in the initial rollout, as opposed to the entire population becoming available at once. Hunt said “how we roll out the boosters will follow time”.
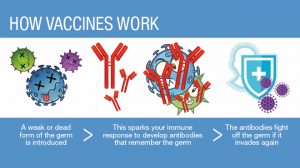
How do vaccines work?
All vaccines, no matter the technology, have the same fundamental goal – to introduce the immune system to an infectious agent, without the risk that comes from disease.
The vaccine needs to follow a similar pathway a virus would have taken to produce an adequate immune response. Viruses enter our cells and use them to replicate themselves. So, the vaccines also need to be delivered in cells where proteins are produced, which mimics a component of the virus itself.
The COVID vaccines all do this by delivering information into our muscle cells, usually in our upper arm. They do this in different ways, such as using mRNA, like Pfizer’s and Moderna’s, or viral vectors, like AstraZeneca’s.
Regardless of the technology, the effect is similar. Our cells use the genetic template in the vaccine to produce the coronavirus’ spike protein, which is a part of the virus that helps it enter our cells. The spike protein is transported to the surface of the cell where it’s detected by the immune cells nearby.
There are also other specialised immune cells nearby, which take up the spike proteins and use them to inform more immune cells – targeting them specifically against COVID.
These immune cells include B cells, which produce antibodies, and T cells, which kill virus-infected cells. They then become long-lasting memory cells, which wait and monitor for the next time it sees a spike protein.
If you’re exposed to the virus, these memory B and T cells allow a faster and larger immune response, destroying the virus before it can cause disease.

So what happens to the vaccine?
Once they’ve initiated the immune response, the vaccines themselves are rapidly broken down and cleared from the body.
The mRNA vaccines consist of a fatty shell, which encapsulates a group of mRNA particles – the genetic recipe for the spike protein. Once this enters a cell, the shell is degraded to harmless fats, and the mRNA is used by the cells to produce spike proteins.
Once the mRNA has been used to produce proteins, it’s broken down and cleared from the cell along with the rest of the mRNAs produced by the normal function of the cell.
In fact, mRNA is very fragile, with the most long lasting only able to survive for a few days. This is why the Pfizer and Moderna vaccines have to be so carefully preserved at ultra-low temperatures.
The vector vaccines (AstraZeneca and Johnson and Johnson) use an adenovirus, which is harmless in humans, as a vector to deliver a genetic template for the spike protein to the cells.

The vector virus has all of its infectious components removed, so it’s unable to multiply or cause disease. Then a genetic template for the spike protein is inserted into the vector.
Once the vaccine is injected, the vector virus binds to your cells and inserts its genetic components, before the shell breaks down and is removed.
The viral machinery gets the genetic template into the control room of the cell, the nucleus, where it takes advantage of our normal protein building activity. The vaccine doesn’t cause any alteration to our DNA.
Normally, this would cause the cell to start producing more copies of the virus, but since this was all removed, all that’s produced is the spike protein.
Again, after making a large amount of the spike, the genetic templates are broken down in a matter of days or weeks.
Does booster shots put everyone else without the booster at risk?
Not necessarily. The urgency behind booster shots for severely immunocompromised people is ensuring all of the vaccinated population has antibodies in their system.
Robert Booy, a University of Sydney professor of vaccinology said that vaccine data had suggested “at least half of severely immunocompromised people may not have had an immune response to either of their first two doses of vaccine”.


“The question is, does it make antibodies and t-cells in your system? The combination of those protect you, because they will provoke your immune system to respond.
“The third dose increases the chance of an effective response in severely immunocompromised people,” Booy said.
It is for this reason that Booy believes most Australians won’t need third doses until at least March next year, before the winter season.
Even older Australians who were vaccinated in the first months of the rollout don’t necessarily require a third dose immediately to be protected, Booy said, because an older immune system alone does not pose the same issues.
How are other countries using boosters?
While Covid vaccine booster rollouts are taking shape in the United Kingdom and the United States, Israel’s vaccine program is the most advanced.
Israel began administering third doses for its general population months ago, and the first data evaluating the impact of its booster program has found that two weeks after more than 1.1 million over-60s had received their third dose, they were 11.3 times less likely to become infected with the Delta variant that currently predominates in Israel and across the world.
As a result, Israel’s government has moved to incorporate booster doses into its vaccine freedom “green pass” system. Green passes are only valid for six months after their second, or third booster shot, or after recovering from Covid.




Does this mean years of booster shots?
It’s unclear, according to Booy, who says there hasn’t been sufficient time for enough real world data.
On Friday, Paul Kelly said: “At the moment, it appears the third dose will be enough, but we’ll just need to see”. The emergence of new Covid-19 variants could influence the need for booster shots into the future.
Booy said governments must work to vaccinate those without an immune response to Covid so far, including their own severely immunocompromised residents as well as the populations of developing nations without significant vaccine uptake.
“It’s people without the benefit of the vaccine where mutations can occur, because it keeps replicating, … and imperfect copies are made more often in immunocompromised people.
“So it’s our local half million of severely immunocompromised people, but also the two billion people in the world who haven’t been vaccinated, before we start giving third doses to people with mildly compromised immune systems in Australia,” he said.




Does everyone need booster shots if vaccinated?
Well, the thing is that COVID vaccines don’t stay in your body for years. A common myth of vaccines that has appeared in recent months is the accusation that they remain active in the body for extended periods of time – a claim which has increased vaccine hesitancy in some people.
However, vaccines are cleared from your body in mere days or weeks. It’s the immune response against the SARS-CoV-2 virus that appears to last for a long time.




This isn’t due to the vaccines themselves remaining in the body. Instead, the vaccines stimulate our immune system and teach it how to respond if we’re ever exposed to the coronavirus.
For the viral vector vaccines, despite ongoing trials, there’s little data available on the duration of the antibody response. The original studies showed efficacy for one to two months, however the duration of protection, and whether a booster will be needed, require further evaluation.